Pros and cons of instillation and inhalation
Both inhalation and instillation are in vivo methods that have their strengths and weaknesses. Being aware of them may help the researcher who has to choose the appropriate method in a scientific and economic way. Therefore, this Section focuses on the differences between the two methods, which are discussed first in the text and then presented in a short form in Table 3 followed by some salient examples.
In a number of ways inhalation exposure is preferable to intratracheal instillation exposure. First, a key advantage of inhalation exposure is that it is the physiological route of exposure to airborne particulates. Second, inhalation considers any effect on the upper respiratory tract, while instillation bypasses upper respiratory tract (e.g. nasal cavity, larynx) and its defence mechanisms. Third, inhalation exposure leads to a more even distribution throughout the lung lobes, while instillation produced highly uneven patterns of lung retention (Brain 1976, Pritchard et al, 1985, Leong et al, 1986, Dorris and Valberg 1992). Fourth, inhalation exposure provides a continuous low deposition and retention rate of test material, while intratracheal instillation delivers an abrupt, concentrated (bolus) dose (Pritchard et al, 1985). This later may overwhelm and overload specific respiratory defence mechanisms and cause more severe lesions (Driscoll et al 1990). Finally, the instillation procedure and liquid per se may produce tissue inflammation not typical of inhalation (Kazmierowski et al, 1977, Driscoll et al, 1990).
However, inhalation exposure requires extensive technical experience and exposure chamber facilities and is expensive. The amount of material that is deposited in the lungs is dependent upon numerous variables, including the aerodynamic diameter and concentration of aerosol particles, the minute ventilation, the breathing pattern, and the disease state of the animals (Brain 1979). These uncertainties may lead to inter-laboratory differences. Another shortcoming is that most particulates have to be micronised by grinding to generate respirable sizes which involves strong mechanical forces and high temperatures and may change particle characteristics.
Instillation technique does not require elaborate exposure chamber and aerosol generation and characterisation equipment. As the equipment required is simple, the technique is inexpensive compared to inhalation exposure. As reproducibility of delivery is highly dependent upon the experience of the individual performing the procedure, appropriate training is essential. Provide that well-trained technicians perform the procedure, the amount of substance delivered is easy to quantify and it is less variable among animals. Thus, intratracheal instillation has been used in many studies as an alternative to inhalation. When substances are very toxic, radioactive or available only in small quantities, instillation may however the only way to examine pulmonary toxicity of substances because it requires significantly less test material and enables safe handling of the test article.
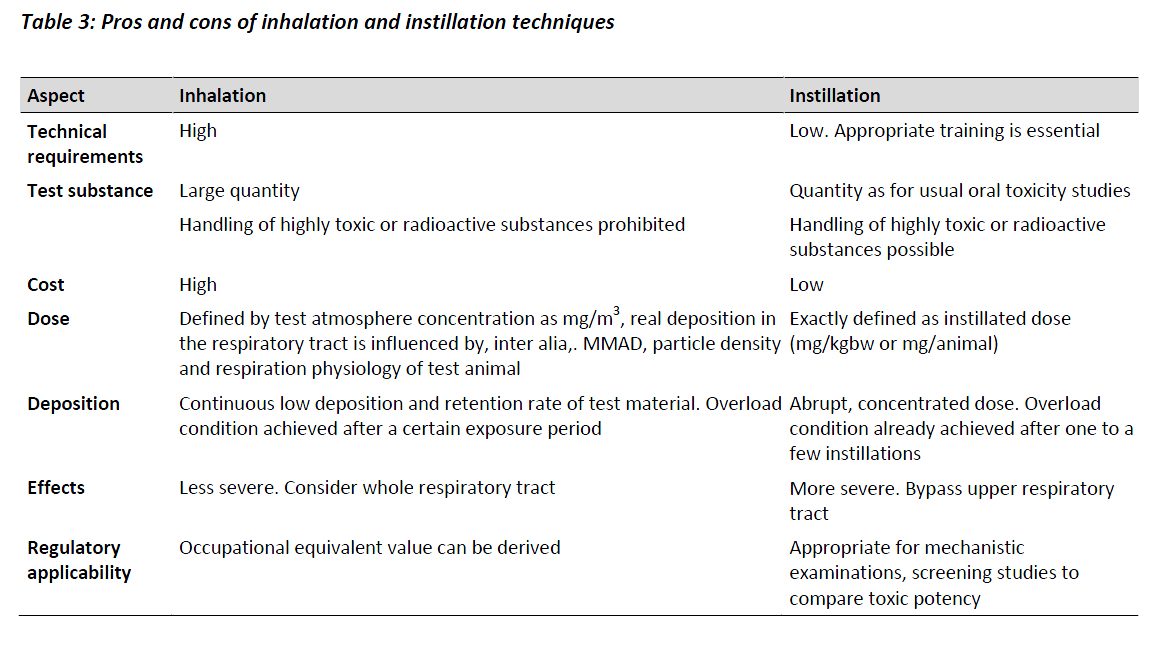
Table 3 summarises the above considerations as follows.
For poorly soluble particles, instillation of quartz and titanium dioxide caused more severe and early effect than inhalation due to the bolus dose (Driscoll et al 1990). However, the type of responses was similar irrespective of the exposure technique. A study conducted by Henderson et al (1995) with the same materials at lower doses/concentrations indicated similarity of the two exposure methods. Interestingly, after inhalation exposure to quartz micro granuloma was observed on pleura surface besides bronchial-associated lymphoid tissue, whereas those formed after instillation was not on pleura surface. This finding indicates that instillation may fail to reveal affected tissue in inhalation study.
A major concern regarding the use of intratracheal instillation is that the introduction of a large bolus dose of the test substance into the lung in a short period of time will overwhelm the normal lung response and defence systems to the extent that it may produce responses that are pathophysiological artefacts that would not be seen if the same dose was delivered over a longer period of time via an inhalation exposure. This can thus produce serious problems for the interpretation of both hazard identification and risk assessment.
Based on their chemical composition as well as their density, surface, mean particle size and behaviour in water Pott and Roller selected 19 different mostly bio persistent dust samples for intratracheal instillation experiments with 2050 female rats in 43 dose (mostly 2 per dust) and 3 control groups (Pott and Roller, 2002). A total of 5 to 20 instillations (once per week) and a broad dose spectrum between 1 and 6 mg per rat and instillation in most cases summed up to a cumulative dose of 30-120 mg dust per rat lung. For quartz, diesel soot, hydrophobic TiO2 (P805) and Ruß, carbon black (Printex 90), smaller doses were used, however with only the latter one fulfilling the criteria for granular biopersistent dust. Unfortunately, with Printex 90 a dosing errors occurred in the lowest dose group (5x1, 5 mg group) by instillation of additional 3 mg dose of ultrafine titanium dioxide. The selection of the highest and the lowest dose level was based on the lifetime particle lung retention of coal miners’ and women in cities in the last decades, respectively. Each exposure experiment comprised a total of 130 weeks after which the rat lungs were examined for tumour incidence and tumour type (Pott and Roller 2002).
Valberg et al, (2009) critically reviewed the outcome of the Pott and Roller study and came to the conclusion that the tumour incidence reflected a saturated inflammatory response due to a rat specific lung overload and is not useful for human risk assessment. The dose selection was based on the assumption that the rat is a miniature human, however, differences in particle translocation (Section 5.7 ) do not allow for this simple dose transformation. With only providing the tumour data the studies do not provide any new information but just show what has been expected to happen with a biopersistent dust in the rat at lung under overload conditions capable of inducing an inflammatory response.
Overall, when testing toxicological impact of occupationally-relevant dusts in animal models, both inhalation of airborne material and intratracheal instillation of fluid-suspended dust into airways may be employed. Although intratracheal instillation is non-physiological and less desirable than inhalation of airborne dust, it may be helpful if certain conditions are met. Keeping in mind that instillation has distinct differences in the distribution, clearance and retention of particles; the doses should not exceed a specific quantity in order to prevent results being dominated by non-specific artefacts. While inhalation studies produce data that can be used for risk assessment, instillation studies are more appropriate when the toxic potency of several materials should be compared.